Moving from assumed to proven chemotherapy benefit - the clarity every patient deserves
The Oncotype DX Breast Recurrence Score® test was developed to help guide chemotherapy treatment decisions based on the prediction of chemotherapy benefit. By revealing tumour biology beyond clinical-pathological parameters, it shifts decision-making from assumed to proven chemotherapy benefit for your HR+, HER2- early-stage breast cancer patients.1-5
Predictive parameters help guide treatment decisions1-2,4,6,12-14
Predictive markers can inform treatment decisions and avoid extrapolation from prognostic factors.6 Predictive markers such as ER and HER2 status identify patients responding to hormonal treatment and trastuzumab, respectively. The Recurrence Score® result informs whether a tumour is likely to respond to chemotherapy. The NSABP B-20 and SWOG 8814 studies established the predictive value of the Recurrence Score® result and the TAILORx study refined the estimates of chemotherapy benefit, identifying two groups of patients:1-3,7-11
- Those who do not benefit from the addition of chemotherapy to endocrine therapy, a majority of early breast cancer patients.
- Those with Recurrence Score® results 26-100 who are most likely to derive substantial benefit from the addition of chemotherapy to endocrine therapy.
Predictive markers can inform treatment decisions1-2,4,6,12-14

The Oncotype DX® test identifies two groups of node-negative patients based on prediction of chemotherapy benefit1-3,7-11

* HR+, HER2-, node-negative, early-stage, invasive breast cancer
a do not benefit from the addition of chemotherapy to endocrine therapy
b significantly benefit from the addition of chemotherapy to endocrine therapy
Prognostic parameters alone cannot guide treatment decisions with precision2,5,15-20
In clinical practice, treatment decisions are often made based on prognostic factors such as tumour size and grade2. However, such clinical-pathological parameters are prognostic and have not been demonstrated to predict chemotherapy benefit.2,5,15 Furthermore, several studies have established that clinical-pathological features cannot predict Recurrence Score®results.2,16-20
Clinical-pathological characteristics do not predict the Recurrence Score® results in TAILORx2
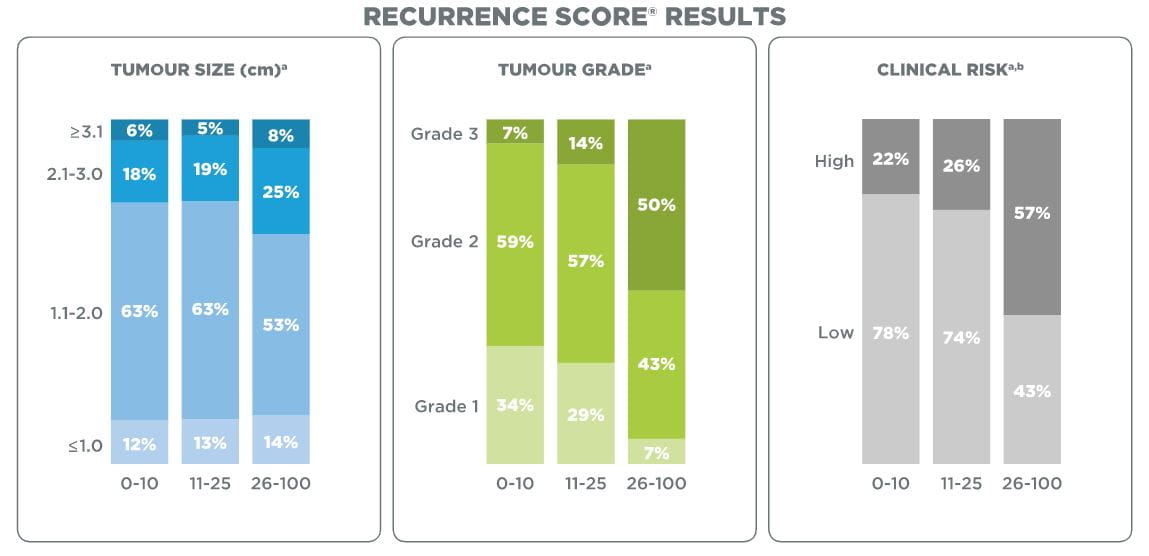
a Patients with unknown values were excluded from the analysis
b Low clinical risk:
tumour size ≤3 cm and Grade 1;
tumour size ≤2 cm and Grade 2;
tumour size ≤1 cm and Grade 3
High clinical risk: all other cases with known values for grade and tumour size
Clinical-pathological features alone cannot predict the Recurrence Score® results in clinical practice16
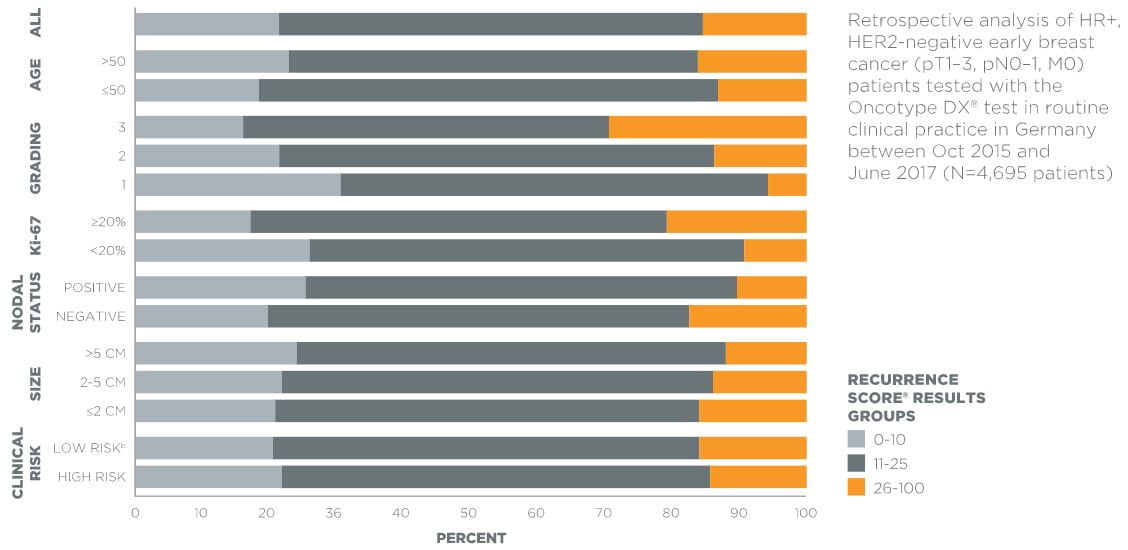
b Low clinical risk:
N0, T ≤3 cm and Grade 1
N0, T ≤2 cm and Grade 2
N0, T ≤1 cm and Grade 3
N1, T ≤2 cm and Grade 1
High clinical risk: all other cases
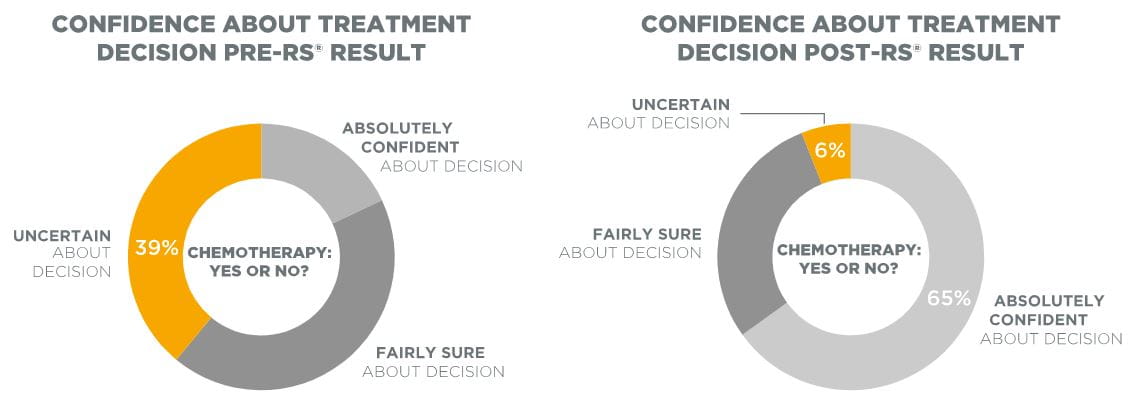
Moreover, relying on these clinical-pathological factors alone was shown to be associated with a high level of uncertainty amongst physicians regarding their treatment decisions. Testing with the Oncotype DX® assay provided greater confidence to clinicians in their treatment recommendations as reflected in a recent case study.17
Uncertainty about treatment decisions based on clinical-pathological features alone17
The Oncotype DX® test can be used to reduce the risk of over- and undertreatment with chemotherapy2,18
The value of the Oncotype DX® test for your HR+, HER2-, node-negative, early-stage breast cancer patients is exemplified by data from the TAILORx trial showing that the Oncotype DX® test aids in the identification of patients who are at risk of over- or undertreatment if clinical pathologic factors alone are used to guide treatment decisions.2,18 Numerous decision-impact studies carried out worldwide in which clinicians accounted for all clinical-pathological features, confirm this potential to reduce the risk of over- or undertreatment with chemotherapy.2,18-21
The Oncotype DX® test reduces the risk of over- and undertreatment2,18

a Low clinical risk: tumour size ≤3 cm and Grade 1; tumour size ≤2 cm and Grade 2; tumour size ≤1 cm and Grade 3
High clinical risk: all other cases with known values for grade and tumour size
b Assuming that adjuvant chemotherapy would have been prescribed or not based on clinical risk.
Decision-impact studies confirm the potential to reduce over- and undertreatment as suggested by TAILORx2,19-21
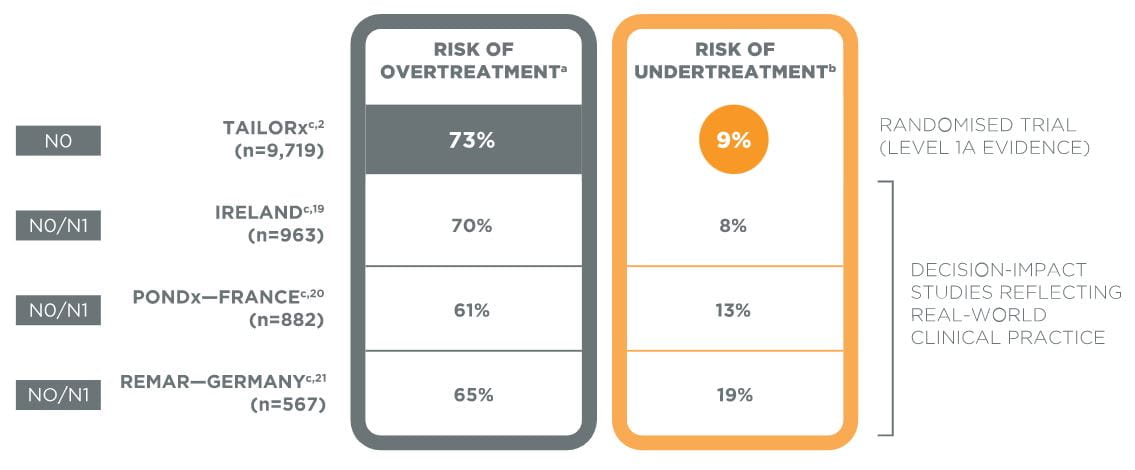
a Percentage of patients initially recommended CT-HT based on all clinical-pathological parameters and de-escalated to HT alone based on RS® result
b Percentage of patients initially recommended HT based on clinical-pathological parameters and escalated to CT-HT based on RS® result
c Patients with unknown values were excluded from the analysis
International guidelines and health technology assessment bodies provide recommendations on whom to test22-26
International guidelines (NCCN, St. Gallen, ASCO)22-24 and health technology assessment (HTA) bodies (IQWIG, NICE)25-26 recognise the Oncotype DX® test for its value in clinical decision-making. Furthermore, they provide guidance on whom to test. The NCCN guidelines recommend to strongly consider all pre- and postmenopausal N0 patients with a tumour size >0.5cm for testing as well as all postmenopausal N1 (1-3 positive nodes) patients22, whereas the German HTA body IQWIG recommends testing all N0 patients when there is treatment uncertainty based on clinical risk assessment25:
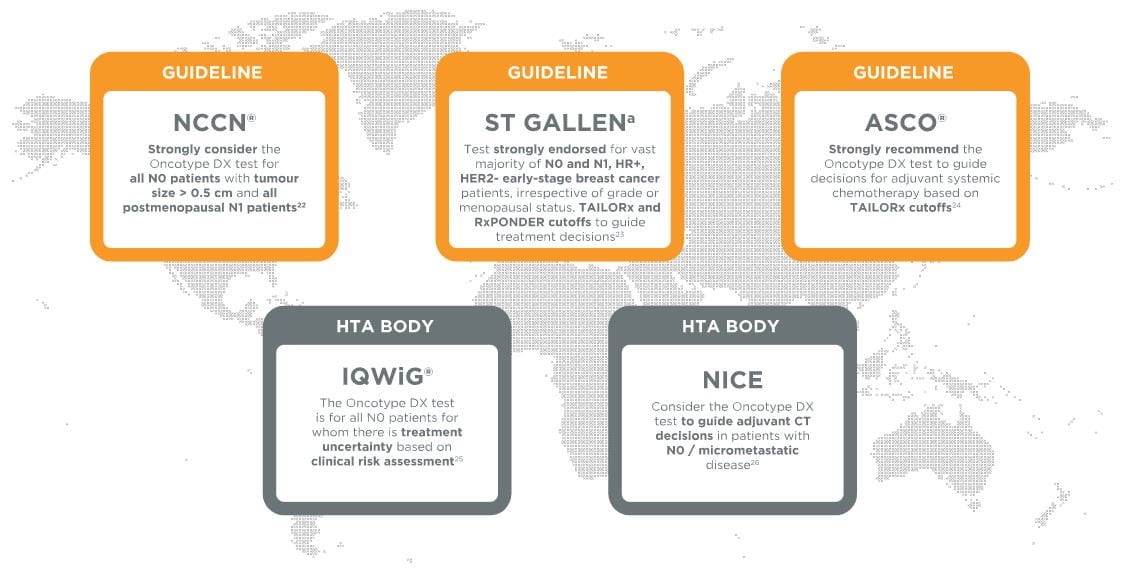
a As voted by a clear majority of the St Gallen International Expert Consensus panel
-
ABBREVIATION
-
REFERENCE